

A guide for how to navigate COVID hospitalization issues, including legal options for worst-case scenarios. Preparation is the best strategy.
DISCLAIMER: This is not medical advice. I’m a lawyer, not a doctor. You should always follow the advice of a trusted physician and make your own independent decisions about your healthcare, especially when it is critical. This guide is presented only as an outline to help inform you about options that may be available.
This is a first draft. I will be refining and expanding this guide, and will post subsequent versions when they are available. If you have any suggestions for improvements to the guide, post them in the comments.
The single most common call we are getting in our office these days is the scenario where a loved-one has been admitted to the hospital, diagnosed with SARS-CoV-2 infection, often attached to a ventilator, and has become concerned about their course of treatment. In many cases the hospitals have refused to release the patient, citing their unstable condition, meaning that at some point, it can become impossible to get off the Covid express.
The most common complaints we get include that patients are being pressured to accept Remdesivir, have been given Remdesivir even though they objected to it, or the hospital will not administer alternative widely-used treatments even though the patient is in critical condition where side effects are less risky than imminent death. I have personally seen hospitals spend tens of thousands of dollars on lawyers to keep patients in their facility.
Here are some suggestions, starting with the time before admission. You should read this now and you might want to bookmark it for later. It could save your life.
## Common Suggestions
[1] Document everything when working with a hospital. Keep or make all paperwork. Take pictures and video of everything. Be organized.
[2] Determine whether you are in a one-party consent or two-party consent state for recordings, and then record meetings with hospital staff. If in a two-party state, you must notify the other party they are being recorded or it may be a felony. Record everything. One option for notice is to just put up a handwritten sign near the patient’s bed notifying folks that recordings are being made for quality assurance. Obviously document the existence of the sign.
[3] Keep a log of the names of all hospital staff involved in the patient’s care.
[4] Before getting anywhere near the hospital, or as soon as you read this if in the hospital, you MUST complete a medical health surrogacy form. This will legally designate the person who can direct your care if you become unable to do so.
Here’s the example form for the State of Florida: http://www.myfloridalegal.com/desigsurrogfaq.pdf
Do some googling for your area.
[5] If you’re in the hospital, or are considering admission, request a copy of the hospital’s current Covid protocol IN WRITING.
[6] Allied doctors have suggested that if you are in the hospital for Covid treatment, the things to focus on are the optimal use of anticoagulants, steroids, and the inpatient setting, meaning the overall day-to-day care (hydration, bedsore prevention, nutrition, etc.).
[7] Consider researching whether you want to receive glucose (sugar water) at all, since some studies suggest this can worsen Covid outcomes. This may be particularly important for diabetics and pre-diabetics. If not, make your wishes known in writing as described above.
[8] If any treating staff — nurses or doctors — make disparaging comments about your vaccination status, directly or indirectly, consider immediately instructing the hospital in writing that person may NOT be involved in your care.
[9] Always remember the old saw about catching more flies with honey. Hospital staff are stressed and unhappy about Covid; I know of many who feel they cannot speak or act freely out of fear of professional reprisal. So the nurse or doctor that you think is an opponent may in fact be an ally willing to help wherever possible, but having to parrot the party line in the meantime. Never show anger or frustration. Keep it together. This is important.
## Emergency Room
The most common scenario that we are hearing is that folks go to the ER for Covid infection and are sent home without treatment if the symptoms aren’t serious enough, and then later are admitted after the patient’s condition has worsened to the point they require hospitalization. An increasing number of reports include folks who go to the ER for a separate reason and wind up testing positive in the ER, or become positive after admission — then get bunged right into the Covid ward and — boom! — they’re on the Covid express.
[1] If you test positive in the ER, whether you were there FOR Covid or for a different reason, and are told you will be admitted, ask about at-home care alternatives. Most corporate hospitals do NOT have home-care protocols. I’ve listed websites below that provide information about alternatives for home treatment. With a little effort, you can find a local doctor or community hospital who will arrange and oversee at-home oxygen if needed.
Ask about the hospital’s Covid protocol BEFORE you agree to be admitted. Is it based on remdesivir and the ventilator? If so, you may want to review the literature on those two treatments before you agree.
[2] If you’re in the ER for a non-Covid critical condition but test positive, you’ll be admitted to the Covid ward. See the notes below, and consider discharging yourself for at-home Covid care the instant your primary issue has been stabilized.
## Pre-Surgery
If you are going in for a non-Covid-related surgery, be aware that nosocomial (hospital-acquired) Covid infections appear to be very common. In other words, even though you are there to have your appendix out, the hospital is going to start testing you for Covid about every ten seconds from the time you arrive until discharge. If you test positive, you’ll be on the Covid express before you know what happened.
It doesn’t matter whether you’ve been vaccinated. You can still test positive and will be treated for Covid infection.
You need to consider this risk in planning your surgery. If you test positive but don’t want remdesivir or ventilation, you need to make that clear in WRITTEN INSTRUCTIONS provided to the hospital IN ADVANCE of your surgery. They need to be part of your medical record. Otherwise you could be on remdesivir even before you come out of anesthesia.
Some people may not have options because of insurance constraints and so forth. Explore your options. And if you DO have options, consider whether your surgery would be better handled in a facility where they don’t also provide Covid treatment, in order to reduce the risk of Covid hospitalization.
Finally, can your surgery be safely deferred? Don’t defer necessary surgery unnecessarily. But if you can wait, that might be a good idea.
## Early Interventions (post-admission)
This section applies to folks or their loved ones who are in the hospital with a Covid diagnosis but remain conscious.
[1] If you haven’t yet received Remdesivir, and DO NOT want it, state that in writing and give it to your doctors. Post a copy by your hospital bed.
[2] If you DO NOT want to be placed on a ventilator, state that in writing and give it to your doctors. Post a copy by your hospital bed.
Be prepared for the hospital to try, hard, to change your mind about those two treatments. This pressure may come when you are weakest. Be ready.
[3] Many people believe that Covid is best treated at home. Your circumstances may vary. Get an opinion from a telemedicine specialist in at-home Covid care like www.jamesclinic.com, or consult www.myfreedoctor.com.
Other online places to check include: aapsonline.org, AFLDS.com, https://covid19criticalcare.com (FLCCC), and GlobalCovidSummit.org.
[4] If you decide that you prefer to treat your Covid at home, or can find a non-corporate independent clinic somewhere that will accept you, discharge yourself. If the hospital pushes back on discharge, you may need to discharge yourself “Against Medical Advice,” or AMA. Ask if your hospital has its own form, otherwise google one.
## Late Interventions
In this section, the patient is no longer conscious or capable of directing their own care. Many times these patients are, unfortunately, already on the ventilator. Therefore relatives or a surrogate are making decisions for the patient. Many patients in this condition are essentially just waiting to die.
[1] If you are concerned about the quality of care, immediately get the hospital’s “Patient Advocate” involved. Most hospitals have one.
[2] Get a second opinion. You’ll need to find a local independent doctor to provide a second treatment opinion. Obviously you will need a doctor who specializes in Covid treatment. You should request the doctor be allowed to evaluate the patient even if they lack admitting privileges for purposes of a second opinion. Request that the doctor be permitted to participate in patient conferences even if by phone.
[3] If at all possible, arrange for someone to be in the room with the patient at all times to ensure consistent high quality of care. At ALL times. Do it in shifts. Even in the middle of the night. Things can happen over the night shift. This person should be checking hydration levels and conferring when possible with nurses and doctors assigned to the patient.
[4] Advocate continually for alternative treatments (iv.mectin, fluvoxamine, and/or monoclonal antibody treatments), if approved by the outside physician.
[5] Some people have successfully arranged to have alternative treatment providers see the patient; or have managed transfers to other hospitals with more flexible Covid treatment, specialized clinics, or even at-home treatment. You may have to insist on the patient being discharged AMA.
[6] Right-To-Try. Consider drug treatments still in clinical trials with right-to-try programs. You MUST use the magic words “I am requesting this against medical advice,” or the hospital will usually reject or ignore your request. Note that iv.mectin and fluvoxamine are APPROVED drugs and are excluded from right-to-try.
For example, one drug in this category that has been frequently mentioned is Zysemi. See (https://tinyurl.com/2p84528z).
[7] You might want to familiarize yourself with successful hospital protocols from 2020, like placing ventilated patients on their stomach.
[8] Your primary goal is to wean the patient off the ventilator. The longer they are on the ventilator, the more likely it is that their condition will continue to deteriorate. Once off the ventilator, you can transition to at-home care.
## Legal Options
[1] Court Options. Court options are limited, and expensive, but have worked in some places. Laws vary widely state-by-state. In Florida, the applicable law is Probate Rule 5.900, which provides for an emergency hearing about patient treatment within 72 hours. My suggestion is that the Court be asked ONLY that the patient (a) be allowed to be treated by the outside physician, or (b) that the patient be released AMA.
As an example, here is a link to Florida Rule 5.900: (https://tinyurl.com/2p8hm8kx).
Your lawyer should carefully consider that asking a Court to order administration of iv.mectin is a risky ask. There have been some successes with this approach, but also many, many failures. Courts have wide latitude in what they can do (or not do) in these situations. Adding a controversial drug into the equation makes the case significantly harder, and since judges are people too, the judge’s preconceived notions about iv.mectin will be a factor. You do NOT want to get into a giant evidentiary battle over the efficacy of iv.mectin.
In other words, simpler and less intrusive requests are more likely to be granted by the Court.
[2] Police Reports. If the patient was given Remdesivir against instructions, that may be a battery, and you might want to consider filing a police report against the hospital and involved staff. If the patient passed away, the stakes are even higher. Although it is hard to say whether the police report will amount to anything, it may be very helpful documentation later. Obviously, provide the police with all paperwork and evidence that you have and keep a file copy of the police report.
I hope this helps. These cases are the worst, most heart-breaking cases I have ever handled in my career. The stakes are literally life-and-death. I don’t mean this guide to be critical of well-meaning doctors and nurses in corporate hospitals — many, if not most are heroic professionals who want the best for patients. Unfortunately, the incentives (e.g. government payments to hospitals) are totally perverse.
Finally, remember that you are not alone! There are more and more advocacy groups forming to help people trapped in hospitals receiving ineffective or harmful treatment. But time is short. The best defense is a good offense; be prepared BEFORE you reach the emergency room.
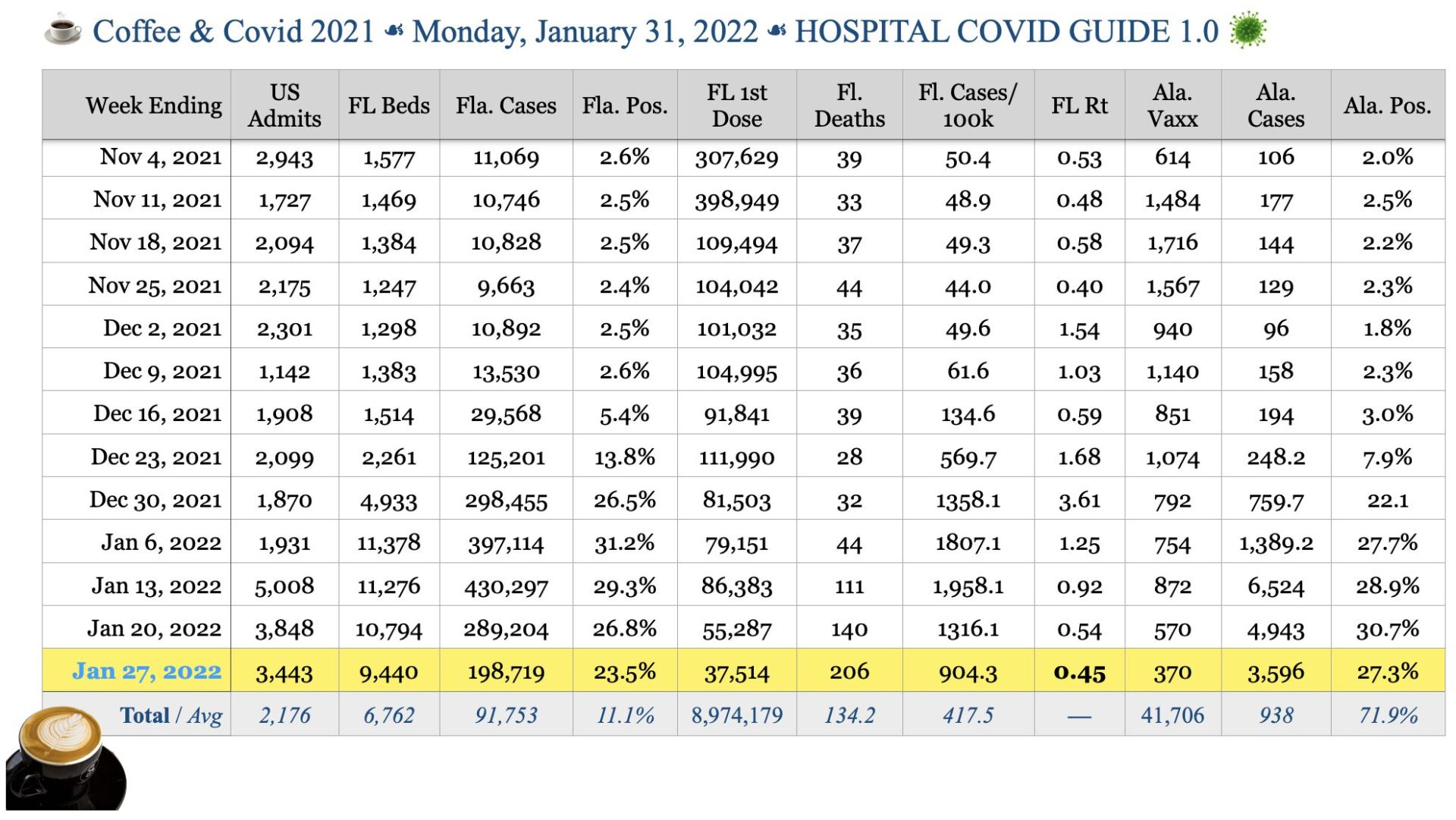
COVID IN FLORIDA AND ALACHUA COUNTY
We have a new weekly report, and it shows what we expected: declining Covid numbers in Florida. I’ll recap the report tomorrow since today’s post is already long, but the data is on the attached chart.
Read Original Article and Updates





{kind=link}
{kind=link}